Home / News / Industry News / Ureteral Stent Set: Components, Types & Clinical Guide
Content
A ureteral stent set is a specialized medical device assembly designed to maintain patency of the ureter, ensuring uninterrupted urine flow from the kidney to the bladder. These sets are indispensable in urological procedures for managing obstructions caused by kidney stones, strictures, or extrinsic compression from tumors. The primary conclusion for clinical efficacy is that the correct selection of stent diameter, length, and material within the set directly influences patient comfort and the risk of complications such as encrustation or migration.
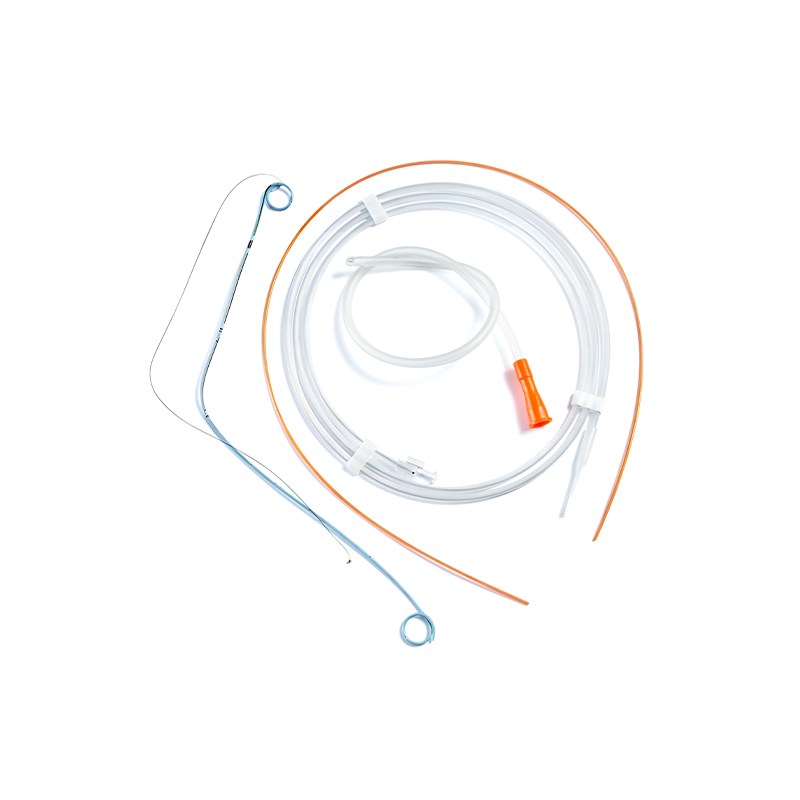
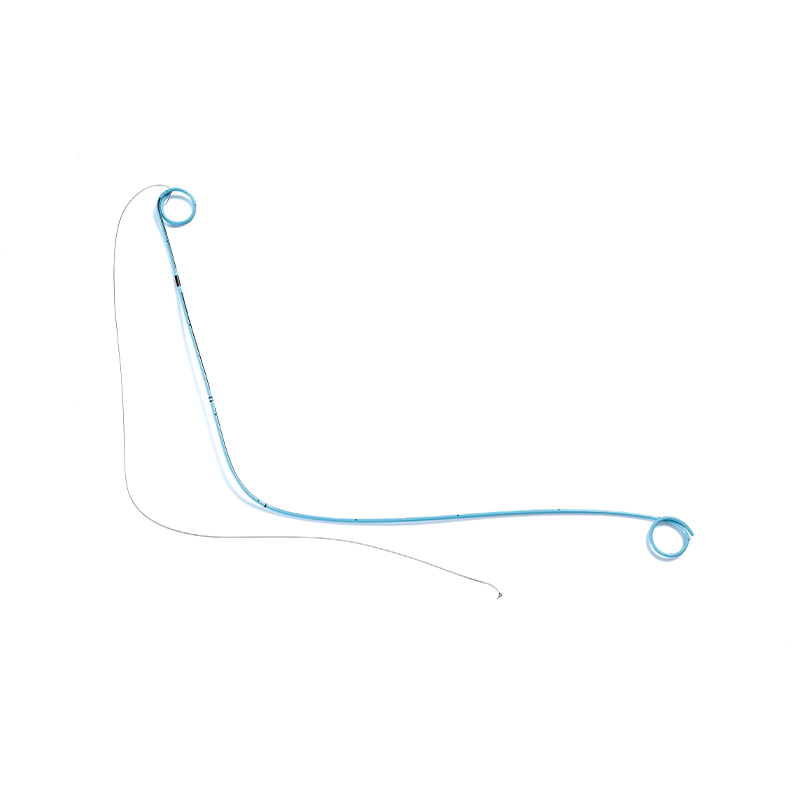
Modern ureteral stent sets typically include the stent itself, a guidewire, and often an introducer or pusher catheter. The standard design features a double-J (DJ) configuration, where coiled ends at both the renal and vesicular positions prevent migration. Materials have evolved from basic polyurethane to advanced hydrophilic coatings and silicone blends, which reduce friction during insertion and minimize biofilm formation, extending the safe indwelling time to 3–6 months for standard polymers and up to 12 months for specialized metallic or coated variants.
Understanding the individual components of a ureteral stent set is crucial for proper handling and insertion. Each element serves a specific mechanical function to ensure safe deployment and secure positioning.
| Component | Function | Key Specification |
|---|---|---|
| Double-J Stent | Maintains ureteral patency | Lengths: 22–30 cm; Diameters: 4.8–7 Fr |
| Guidewire | Provides track for stent advancement | Hydrophilic tip, 0.035–0.038 inch diameter |
| Pusher Catheter | Advances stent over guidewire | Radiopaque markers for positioning |
| String (Optional) | Facilitates non-cystoscopic removal | Attached to vesical coil, exits urethra |
Selecting the correct stent size is critical to avoid complications. A stent that is too long may cause irritative voiding symptoms due to the distal coil poking the bladder wall, while one that is too short risks migrating into the ureter. Standard adult lengths range from 24 cm to 28 cm, determined by patient height and anatomical measurements via pre-operative imaging. Diameter selection (typically 6 Fr or 7 Fr) balances drainage efficiency with patient comfort; larger diameters offer better flow but may increase discomfort and hematuria.
The material composition of the ureteral stent set significantly impacts its performance, particularly regarding encrustation and infection resistance. Traditional materials are being replaced by advanced polymers designed to withstand the harsh urinary environment.
Proper insertion of a ureteral stent set requires precision to minimize trauma and ensure correct positioning. The procedure is typically performed cystoscopically under fluoroscopic guidance.
Patients with indwelling stents often experience irritative symptoms such as frequency, urgency, and flank pain during voiding due to vesicoureteral reflux. Prophylactic antibiotics may be prescribed to prevent infection. It is crucial to schedule timely removal or exchange, as forgotten stents can lead to severe encrustation, stone formation, and potential loss of kidney function. Regular follow-up imaging ensures the stent remains patent and properly positioned.
Product Categories
Contact Us

+86-571-87687066
+86-18106505367

Workshop 1, 1st Floor(Zone B), 3rd Floor; Office Building 3rd&4th Floors, No. 550 Yinhai Street, Baiyang Sub-district, Qiantang District, Hangzhou City, Zhejiang Province, P.R.China
Ready to Begin?
Get in Touch

Now!
sungood
 English
English Español
Español