Home / News / Industry News / Laryngeal Mask Airway Guide: Insertion, Sizing & Safety Tips
Content
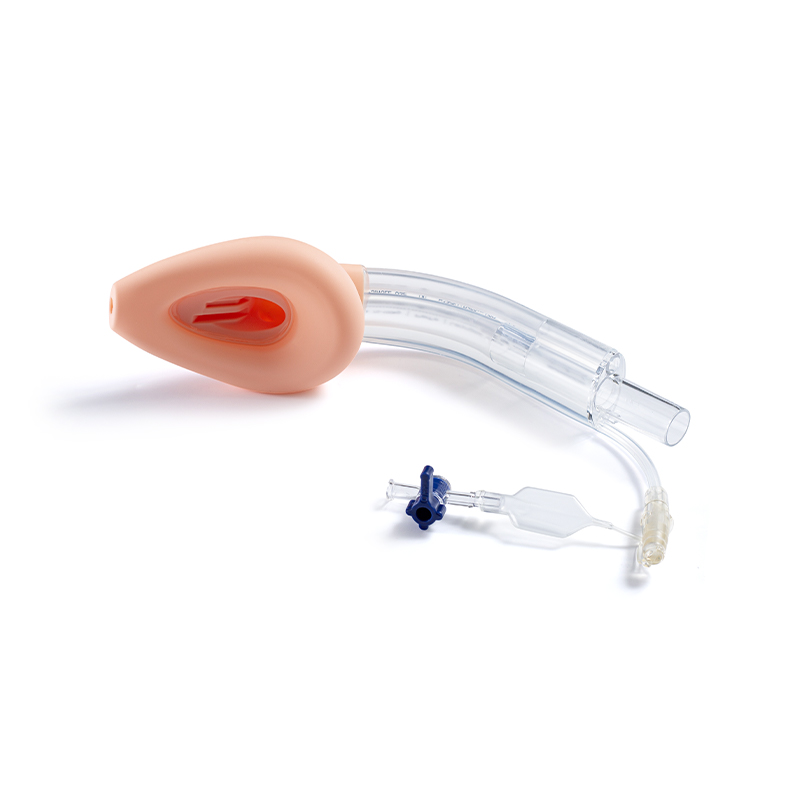
The Laryngeal Mask Airway (LMA) is a supraglottic airway device that has revolutionized anesthesia and emergency airway management by offering a less invasive alternative to endotracheal intubation. Correct sizing and cuff pressure maintenance below 60 cm H2O are the two most critical factors in preventing complications such as sore throat, nerve injury, and inadequate ventilation. This article provides a practical, evidence-based guide to selecting, inserting, and managing an LMA safely in clinical settings.
Proper sizing is essential for achieving an effective seal and minimizing trauma. An LMA that is too small may leak under positive pressure ventilation, while one that is too large can cause pharyngeal trauma or postoperative dysphagia. Selection is primarily based on patient weight, but anatomical variations should always be considered.
| LMA Size | Patient Weight (kg) | Max Cuff Volume (ml) |
|---|---|---|
| Size 1 | < 5 kg (Neonate/Infant) | 4 ml |
| Size 2 | 5 - 10 kg (Infant) | 10 ml |
| Size 2.5 | 10 - 20 kg (Child) | 14 ml |
| Size 3 | 20 - 30 kg (Child) | 20 ml |
| Size 4 | 30 - 50 kg (Small Adult) | 30 ml |
| Size 5 | 50 - 70 kg (Adult) | 40 ml |
| Size 6 | > 70 kg (Large Adult) | 50 ml |
Clinical Tip: If a patient falls on the border of two sizes, it is generally safer to choose the larger size for a better seal, provided it can be inserted without excessive force.
Successful placement of the Laryngeal Mask Airway requires adequate depth of anesthesia or sedation to suppress laryngeal reflexes. The classic insertion method involves a rotational movement to navigate the device around the tongue and into the hypopharynx.
Deflate the cuff completely to ensure a smooth profile. Apply a water-soluble lubricant to the back of the cuff (away from the aperture bars) to facilitate passage. Avoid over-lubrication, which can cause the device to slip out or obstruct the view.
Once inserted, the cuff must be inflated to create a seal. However, overinflation is a common error that leads to complications. Intracuff pressure should never exceed 60 cm H2O, as higher pressures can compress the lingual, hypoglossal, and recurrent laryngeal nerves, potentially causing temporary or permanent nerve palsy.
After inflation, perform a leak test by delivering positive pressure ventilation. A slight leak at peak inspiratory pressure is acceptable and often desirable to prevent gastric insufflation. If the leak is excessive, reposition the head or adjust the cuff volume. If ventilation remains difficult, do not repeatedly attempt to use the LMA; proceed to endotracheal intubation.
While the Laryngeal Mask Airway is versatile, it does not protect the airway from aspiration as effectively as an endotracheal tube. Therefore, patient selection is crucial.
The Laryngeal Mask Airway is a vital tool in modern airway management, offering a balance between ease of use and patient safety. Success depends on meticulous attention to sizing, gentle insertion technique, and strict control of cuff pressures. By adhering to these guidelines, clinicians can minimize complications and ensure effective ventilation for patients undergoing short-to-moderate duration procedures. Always have a backup plan for difficult airways, including equipment for immediate endotracheal intubation.

Product Categories
Contact Us

+86-571-87687066
+86-18106505367

Workshop 1, 1st Floor(Zone B), 3rd Floor; Office Building 3rd&amp;4th Floors, No. 550 Yinhai Street, Baiyang Sub-district, Qiantang District, Hangzhou City, Zhejiang Province, P.R.China
Ready to Begin?
Get in Touch

Now!
sungood
 English
English Español
Español